Table of contents
Early-phase cell and gene therapy (CGT) product development focuses primarily on product safety issues. However, it is also critical to demonstrate the firm’s capability to consistently and reproducibly manufacture its investigational product.
At the ISPE Annual Meeting held in Orlando, Florida, in early November 2022, Center for Biologics Evaluation and Research (CBER) Office of Tissues and Advanced Therapies (OTAT) Division of Cellular and Gene Therapies Branch Chief Melanie Eacho discussed common issues her office sees in early phase development and in Biologics License Applications (BLAs) submitted for approval.
(See “A Deep Dive into Cell and Gene Therapy Regulatory Considerations: Part One” for insights into FDA’s New Office of Therapeutic Products.)
Common issues in early phase studies mainly focus on product safety issues, which she explained include methodology, controls and reference standards for release assays, and qualification of dose measurement assays and the differences between those used for preclinical and clinical studies.
Reagent qualification is a common topic “that we go back and forth on with sponsors with,” Eacho said.
Common CMC Issues Explained
Eacho provided her recommendations on the content of the Chemistry, Manufacturing, and Control (CMC) section of the application and shared common problems she has seen in the applications.
CMC Information provided in an Investigational New Drug (IND) Application, Eacho explained:
- Should include information that describes the composition, manufacture, and control of the investigational product
- Should be sufficient to assure identity, quality, purity, and potency (biological activity) of the investigational product
- Early phase is more focused on safety: identity, purity, and activity
- Later phases require more information on quality and potency
The amount of information the agency will find sufficient will depend on the phase and scope of the initial clinical investigation. As development proceeds, it will be necessary to supplement initial CMC information as appropriate to address the expanded phase and scope of clinical investigations.
Some product safety issues to consider:
- Release assays: methodology, controls/reference standards
- Method for sterility, mycoplasma? Rapid? Qualified?
- Dose measurement assay: different for preclinical studies than for clinical studies; qualified?
- Critical raw materials and reagents: source, documentation, CoA
- Delivery device: regulatory status? Investigational? Is it compatible with the drug product?
- Donor eligibility
Donor Screening and Testing
Regarding donor testing and screening, for allogeneic products, donor testing and screening must be done per the requirements in 21 CFR 1271. CBER guidance documents provide additional detail on what communicable disease agents must be tested, when donors must be tested, where the testing must take place, and how they are tested, including the types of test kits.
The two elements of donor eligibility are screening and testing. Donor screening is done using medical questionnaires and subjects’ medical records. Donor specimens are tested. Testing of donor specimens must be done using FDA-licensed kits at Clinical Laboratory Improvement Amendments (CLIA)-certified labs using FDA-cleared or approved kits specifically for that purpose.
Up-to-date information on test kits is available on the FDA website, including guidance documents that provide additional detail on the following:
- What communicable disease agents must be tested
- When donors must be tested
- How they are tested and the types of test kits, and
- Where the testing must take place
“The variety of disease agents that must be tested or screened for is a common issue that requires a lot of back and forth during review,” Eacho emphasized, “especially when donor materials previously acquired a lot of cases for things like Induced pluripotent stem cell (iPSC)-based disease modeling and the cell replacement therapy where you already have your clones made and banked, and also when your donor material is from foreign locations and some of these testing and CLIA certified labs aren’t available.”
It is important to remember that in the case of autologous starting material if screening and testing per 1271 are not being conducted, special labeling requirements are needed on autologous products.
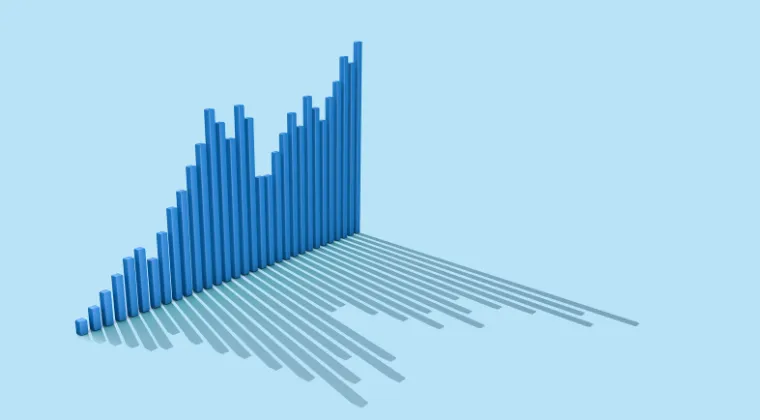
The historical data: 21 CFR 1271 Trends from Redica Systems
Using Redica Systems, we looked at the last five years (2018-2022) to see trends for subsequent sections of 21 CFR 1271.
This part of the CFR is that which governs “Human Cells, Tissues, and Cellular and Tissue-Based Products.”
To gather this data went to the Reports tab and ran the CFR Citation Report. This report allows your team to review citations over different periods within minutes.
The following chart shows the top five cited sections within 21 CFR 1271. The leader for the group is 1271.47, which covers “What procedures must I establish and maintain?”.
Schedule a working session with us to view the full breakdown of subsections within the CFR group! We’d be happy to walk you through this data set and others.

Reagents Cause Discussion
The reagents used in manufacturing – including, for example, serum albumin – are a frequent topic of communication between early-phase CGT product developers and the agency.
FDA recommends that manufacturers use the highest quality reagent available. This can include research-grade reagents, if properly qualified, which is often done by the sponsor or the manufacturer.
For all human, animal, and even insect-provided reagents, there are myriad considerations from donor eligibility, obviously for human products, but also just adventitious agent testing that is specific to different species.
All reagents should be qualified. If the vendor is missing information on certain tests, the expectation is that the manufacturer of the product is ultimately responsible in obtaining or conducting the missing tests.
If the reagent vendor has a master file with FDA for the specific reagent, the agency recommends that the vendor provide a letter of authorization authorizing the applicant to cross-reference the master file submission.
Here is a listing of some of the different concerns that FDA sees with the types of different reagents encountered during application review:
Human-derived materials
- Human serum albumin – need to use U.S. licensed product
- Autologous or pooled human serum – comply with donor eligibility
Animal-derived materials
- Adventitious (viral) agents
- BSE/TSE issues for bovine products require attention to the country of origin and age of the herd
- “Serum-free” media does not necessarily mitigate the concern
Key takeaways:
- Common issues in early-phase CGT studies mainly focus on product safety issues
- Reagent qualification is a common topic “that we go back and forth on with sponsors with”
- As development proceeds, it will be necessary to supplement initial CMC information as appropriate to address the expanded phase and scope of clinical investigations.
- “The variety of disease agents that must be tested or screened for is a common issue that requires a lot of back and forth during review”
- Redica Systems data shows that 21 CFR 1271.47 is the most cited within 21 CFR 1271 from 2018 – 2022
- FDA recommends that manufacturers use the highest quality reagent available
Stay tuned for two subsequent parts of this article detailing the insights Eacho provided:
- Part Three: GCT Product CQAs, Lot Release, Device Considerations
- Part Four: CMC Expectations And Challenges In Late Phase Development.